 This information is intended for healthcare professionals based in Ireland.
If you are not a healthcare professional in Ireland, click here
This information is intended for healthcare professionals based in Ireland.
If you are not a healthcare professional in Ireland, click here
This information is intended for healthcare professionals based in Ireland.
If you are not a healthcare professional in Ireland, click here
NVAF Real-World Data
ELIQUIS® (apixaban) RCT results, complemented by real-world evidence1,2
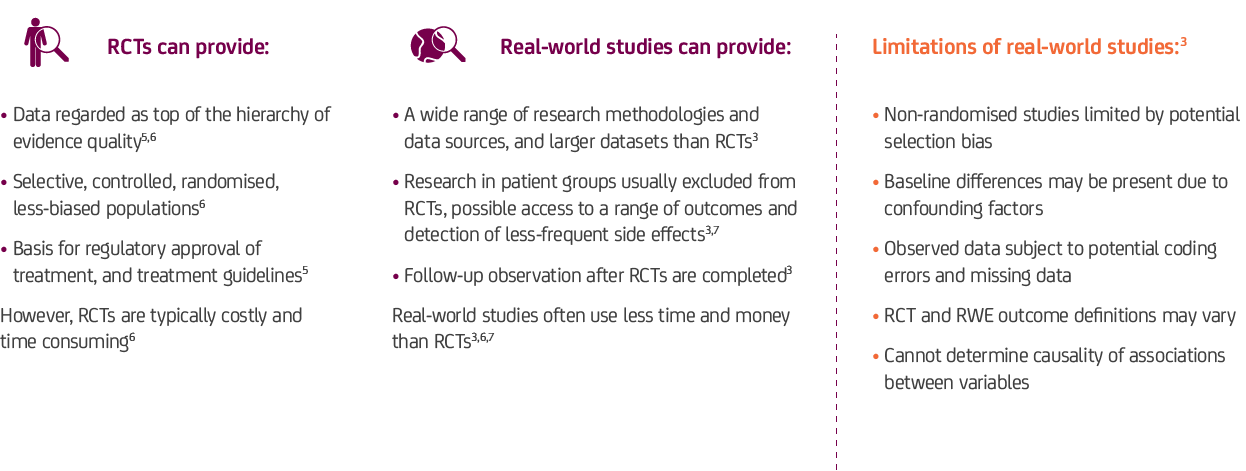
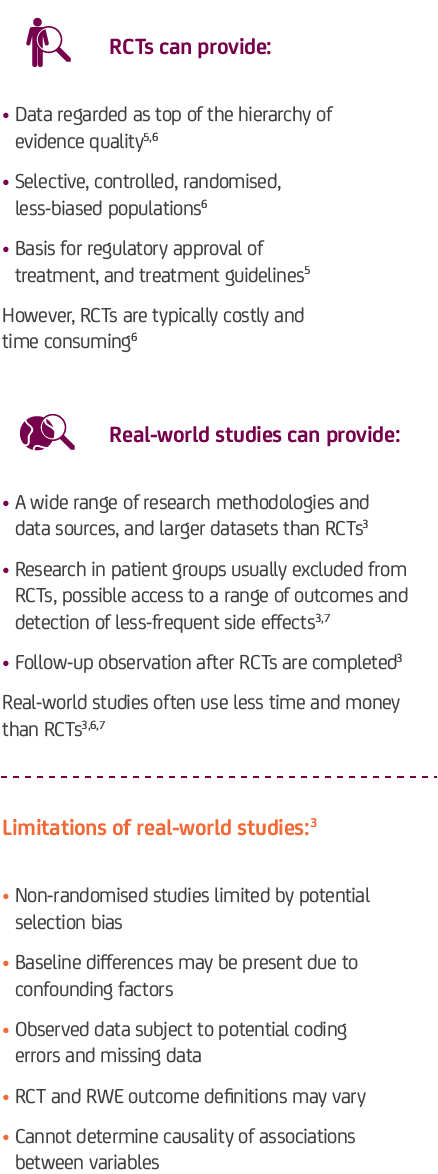
Real-world evidence complements RCTs by providing key insights into diverse clinical settings and patient populations1,3,4
Summary of differences between clinical trials vs. real-world studies3
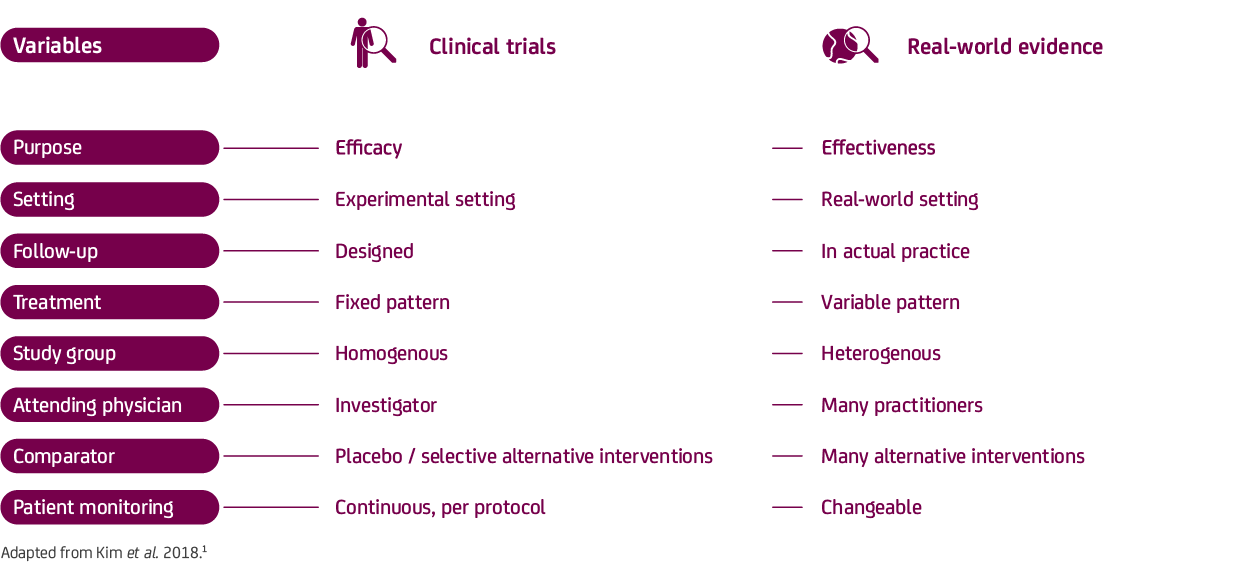
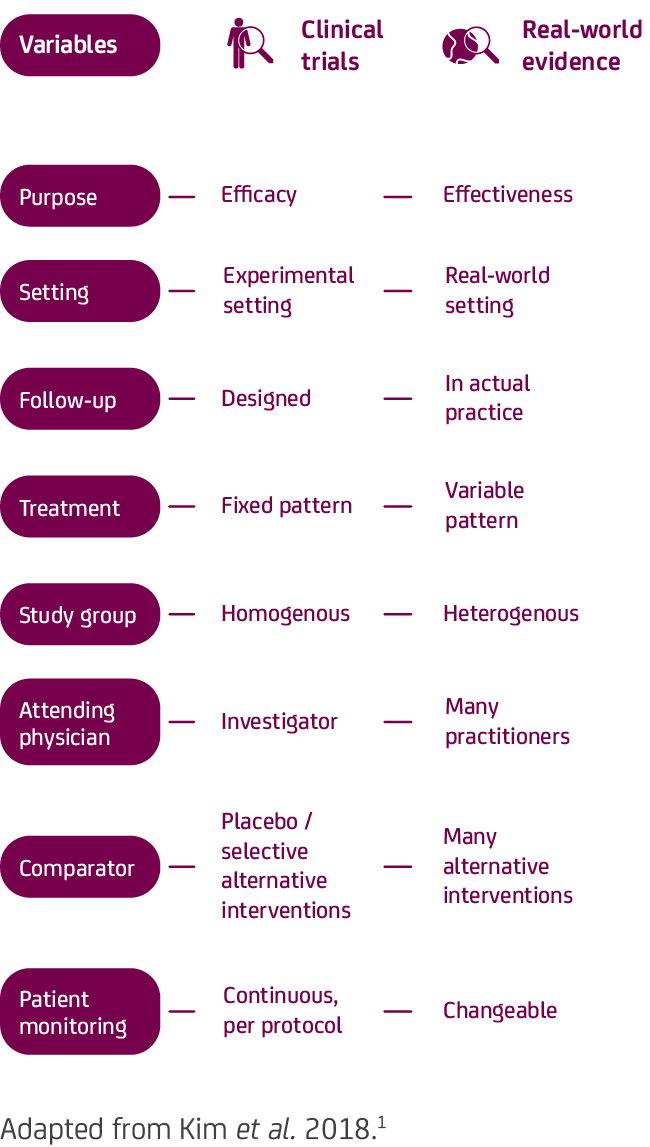
RCTs are the ‘gold standard’ for determining the efficacy and safety of a medicine, while real-world evidence can provide insight into the effectiveness in routine clinical practice – together, these can support treatment decisions1,3,4
Rationale and study overview
ARISTOPHANES was a large-scale retrospective, US real-world analysis examining both DOAC vs. warfarin, and DOAC vs. DOAC in 434,046 propensity score - matched patients with NVAF.2
Study population:2
- Adult patients with a diagnosis of AF and a first OAC prescription in the study period (1 January 2013 to 30 September 2015)* and no OAC exposure for 12 months prior
- Pooled population from US Medicare and four US commercial claims databases†
Objective:2‡
- To compare the rates of stroke / systemic embolism and major bleeding across various subgroups among patients with NVAF newly prescribed ELIQUIS, rivaroxaban, dabigatran, or warfarin
Outcomes:2
- Effectiveness outcome: time to first stroke / systemic embolism (including ischaemic stroke, haemorrhagic stroke, and systemic embolism)
- Safety outcome: time to first major bleed (including gastrointestinal bleeding, intracranial haemorrhage, and major bleeding at other sites)
Analysis:2
- Retrospective cohort analysis, using Cox proportional hazard regression to evaluate outcomes across propensity score-matched cohorts§
- Follow-up period: 30 days after discontinuation date, switch date, death, end of continuous medical or pharmacy plan enrolment, or end of study period (whichever occurred first)
What are the limitations of the ARISTOPHANES real-world analysis?2
- Only statistical association rather than causal relationships could be inferred
- Although cohorts were propensity score matched, potential residual confounders exist, which are not available in the dataset – this limitation is especially important for interpreting DOAC vs. DOAC, which are for hypothesis generation given the lack of head-to-head trials
- Outcomes were identified using ICD-9-CM codes, without further adjudication using precise clinical criteria or further validation against healthcare providers’ medical records
- There was no evaluation of the dose-reduction criteria for DOACs due to the absence of comprehensive data on body weight or serum creatinine / creatinine clearance
- Laboratory values, such as INR measurements, are not available in the database, therefore it is not possible to determine time in therapeutic range for patient prescribed warfarin
- Many clinically important outcomes, such as mild-to-moderate bleeding associated with oral anticoagulant use were not evaluated because they cannot be reliably measured in claims databases
- The study relied on prescription dispense records to characterise anticoagulant drug exposure, but patients’ actual drug-taking behaviours could not be measured
- Observed and unobserved heterogeneity may exist across the 5 data sources
- There is no guarantee that patients were dosed according to the US prescribing information for each DOAC and warfarin
- Results may not be generalisable to the overall NVAF population in the US because the study did not include uninsured patients and patients solely covered by other public health insurance plans
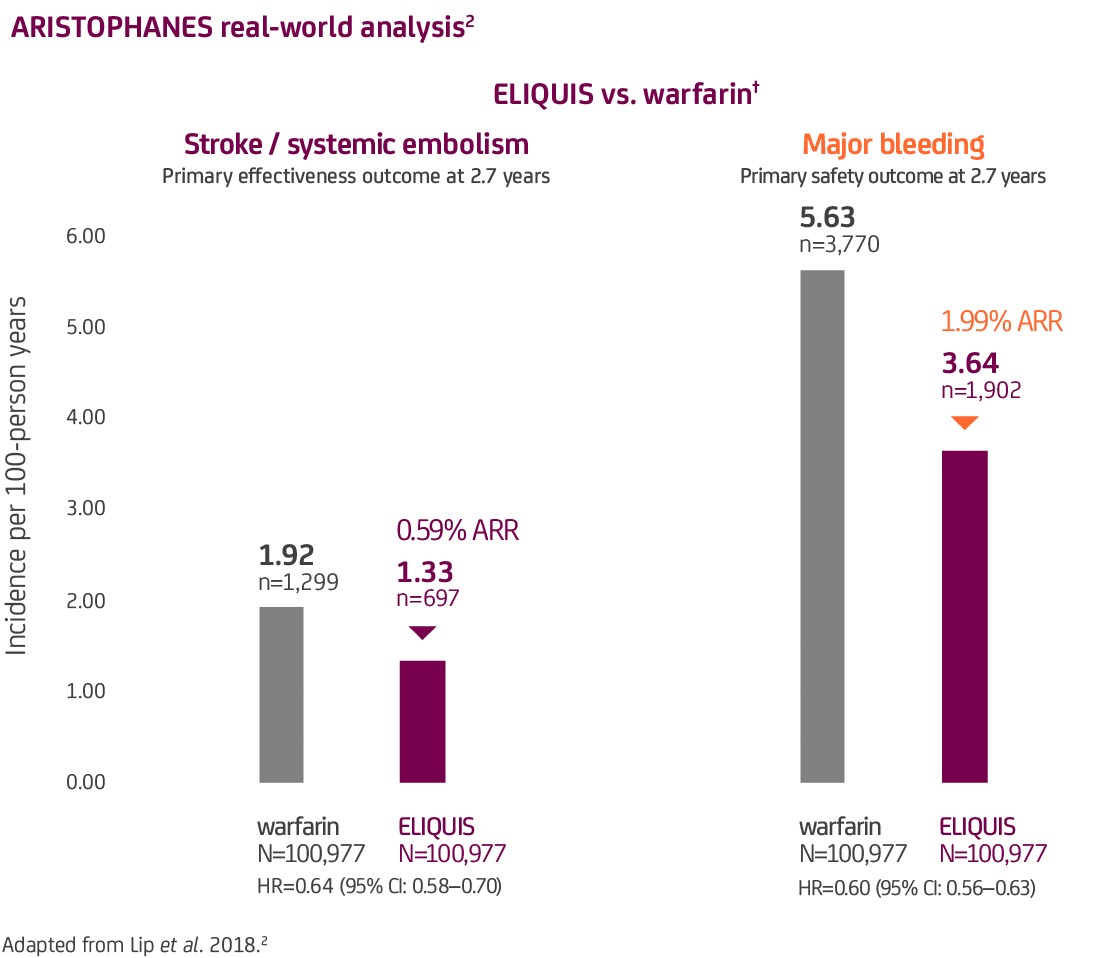
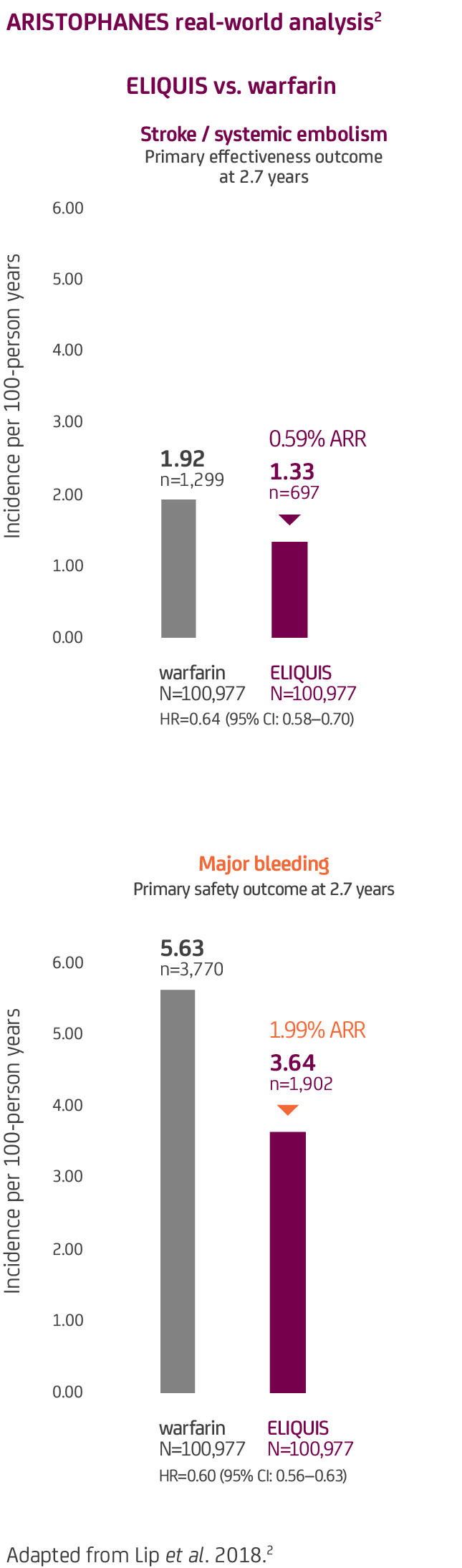
 ELIQUIS was associated with a reduced risk of stroke / systemic embolism and a favourable bleeding profile across different outcomes vs. warfarin in real-world settings2#
ELIQUIS was associated with a reduced risk of stroke / systemic embolism and a favourable bleeding profile across different outcomes vs. warfarin in real-world settings2#
There are no head-to-head RCTs comparing the DOACs.
The results of the ARISTOPHANES real-world analysis should only be used for hypothesis generation and must be interpreted with caution, as the effectiveness and safety outcomes and assessed patient populations may be different to those in the ARISTOTLE clinical trial.
Additional real-world data studies are available. Please click GET IN TOUCH to contact your local BMS / Pfizer representative for more information.
ELIQUIS (apixaban) is indicated for prevention of stroke and systemic embolism in adult patients with non-valvular atrial fibrillation (NVAF), with one or more risk factors, such as prior stroke or transient ischaemic attack (TIA), age ≥75 years, hypertension, diabetes mellitus, symptomatic heart failure (NYHA Class ≥II); treatment of deep vein thrombosis (DVT) and pulmonary embolism (PE), and prevention of recurrent DVT and PE in adults; and, prevention of VTE in adult patients who have undergone elective hip or knee replacement surgery.8
Footnotes:
- * End date was selected as it was the last date before the US moved from ICD-9 codes to ICD-10 codes. Due to this coding switch, it is believed that the researchers wanted to keep the outcome definitions consistent.
- † Data in this study were pooled from the US Centres for Medicare and Medicaid Services Medicare data, and 4 commercial claims databases in the US: Truven MarketScan®, IMS PharmMetrics Plus™, Optum® Clinformatics® Data Mart, and the Humana Research Database.2 Though commercial datasets may contain duplicate patient records when pooled, the number of duplicate is likely to be small (~0.5%) and therefore unlikely to affect the results.9
- ‡ Outcomes were based on hospitalisations with stroke / systemic embolism as the principal or first-listed diagnosis.2
- § Patients were matched 1:1 in each dataset, using propensity scores generated by logistic regression based on demographics, CCI score, baseline bleeding and stroke / systemic embolism history, comorbidities, and baseline co-medications.
- # In the ARISTOPHANES retrospective, US real-world analysis, the primary effectiveness outcome was time to first stroke / systemic embolism including ischaemic stroke, haemorrhagic stroke, and systemic embolism. The primary safety outcome was time to first major bleed, including gastrointestinal bleeding, intracranial bleeding, and bleeding from other sites.2 Outcomes were based on hospitalisations with stroke / systemic embolism or major bleeding listed as the principal or first-listed diagnosis, as identified using ICD-9 codes.2 After propensity score matching in the ARISTOPHANES retrospective, US real-world analysis, (ELIQUIS vs. warfarin), 75.4% of ELIQUIS patients received the standard dose of ELIQUIS 5 mg BD and 24.6% of patients received a reduced dose of ELIQUIS 2.5 mg BD.2
- BD = Twice Daily CCI = Charlson Comorbidity Index CI = Confidence Interval DOAC = Direct-acting Oral Anticoagulant HR = Hazard Ratio GI = Gastrointestinal ICH = Intracerebral Haemorrhage
- ICD-9 = International Classification of Diseases, Ninth Revision INR = International Normalised Ratio N = Total number of patients in either the ELIQUIS group or the warfarin group n = Number of patients with event NVAF = Non-Valvular Atrial Fibrillation OAC = Oral Anticoagulant RCT = Randomised Controlled Trial RWE = Real-World Evidence
References:
- Granger CB et al. N Engl J Med 2011; 365: 981–992.
- Lip GYH et al. Stroke 2018; 49: 2933–2944.
- Kim HS et al. J Korean Med Sci 2018; 33: e213.
- Frost CE et al. Br J Clin Pharmacol 2013; 76: 776–786.
- ABPI. The vision for real-world data: harnessing the opportunities in the UK.
- ABPI. Demonstrating value with real world data: a practical guide.
- Camm AJ et al. Open Heart 2018; 5: e000788.
- ELIQUIS® (apixaban) Summary of Product Characteristics
- Lip GYH et al. Stroke 2018; 49: 2933–2944. Online supplement.
Reporting of suspected adverse reactions after authorisation of the medicinal product is important. It allows continued monitoring of the benefit/risk balance of the medicinal product. Healthcare professionals are asked to report any suspected adverse reactions via HPRA Pharmacovigilance at www.hpra.ie
Adverse reactions should also be reported to Bristol-Myers Squibb Medical Information on 1 800 749 749 or medical.information@bms.com